
TL;DR
- What it is: A five-step framework for approaching any rash, organized by morphology, distribution, etiology, and treatment.
- First question to ask: What does this lesion look like?
- Don’t miss: Petechial and purpuric rashes are non-blanching. These patients need more attention, with a deeper workup and earlier referral timeframe.
- Treatment logic: Four buckets: steroid-responsive, antifungal, antibiotic, or supportive only.
- Free resource: Download the Blox Rash Guide for a full visual reference by morphology, distribution, and treatment.
Have you ever seen someone check in with a “rash” and thought “please just let this be poison ivy”? Yeah, same. Rashes can feel overwhelming, especially when half of them look the same. But if you have a standard approach you can use for every patient, they become a lot more manageable.
Here’s a simple approach you can use every day, and the one we built the Blox Rash Guide around.
Step 1: What’s It Look Like?
Before you do anything else, describe what you’re looking at. This sounds basic, and it is, but it’s also easy to get overwhelmed with a full clinic where every patient needs something different.
There are seven primary lesion types that cover the vast majority of what you’ll see:
- Maculopapular: Flat or raised red/pink spots. Think viral exanthem, drug rash.
- Scaly: Dry, flaky surface, often patchy or annular. Think tinea, psoriasis, eczema.
- Vesicular/Bullous: Fluid-filled lesions. Think HSV, zoster, bullous pemphigoid.
- Pustular: Pus-filled lesions. Think folliculitis, impetigo, candidiasis.
- Petechial/Purpuric: Non-blanching red or purple spots. Think meningococcemia, vasculitis, RMSF.
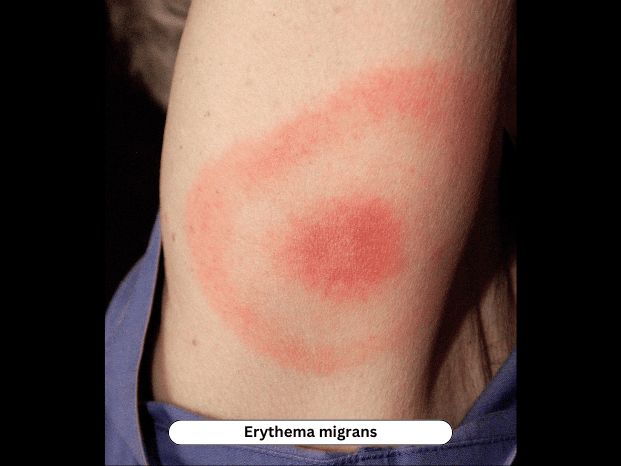
- Targetoid: Concentric ring or bull’s-eye lesions. Think erythema multiforme, Lyme disease.
- Urticarial: Transient wheals with central clearing. Think allergic reaction, viral trigger.
The reason I start with morphology is that it immediately narrows my differential and gives me a manageable starting point to work from.
Step 2: Where’s It At?
Once I know what it looks like, I look at where it is.
- Face: Seborrheic dermatitis, impetigo, lupus
- Palms and soles: RMSF, secondary syphilis, hand-foot-mouth, Kawasaki disease
- Trunk: Pityriasis rosea, drug eruptions, viral exanthem
- Intertriginous areas: Candida, erythrasma, inverse psoriasis
- Extremities: Tinea, scabies, RMSF (early), contact dermatitis
- Generalized: Viral exanthem, drug reactions, atopic dermatitis
Rashes on the palms and soles include a short list with some serious names on it (syphilis, RMSF, etc.) so make sure to take your time with these patients. And anything unilateral in a dermatomal distribution should make you think zoster, even if they just have pain without a true rash yet.
Step 3: Narrow to Likely Etiology
Once I’ve figured out what it looks like and where it’s at, I’m sorting into one of four buckets:
- Infectious: Viral, bacterial, or fungal
- Inflammatory: Eczema, psoriasis, seborrheic dermatitis
- Allergic/Immune: Contact dermatitis, urticaria, erythema multiforme
- Autoimmune/Other: Lupus, dermatomyositis, vasculitis
This is where your history can help. You have to ask specifically about new meds, tick exposure, sick contacts, and sexual history (yes it can be awkward, do it anyway). A symmetric, non-itchy rash on the trunk, palms, and soles in a younger patient is secondary syphilis until you rule it out.
Step 4: Treat the Category
This part is actually pretty easy once you’ve gone through Step 1-3.
- Steroid-responsive: Eczema, contact dermatitis, psoriasis, allergic or immune-mediated rashes.
- Triamcinolone 0.1% is an easy go-to for most body sites.
- Clobetasol 0.05% does well for thick plaques or areas like the soles of feet.
- Try to avoid high-potency steroids on the face or in skin folds, and all patients need education on using these for short periods of time.
- Antifungal: Tinea and candidiasis.
- One thing to be mindful of: tinea may initially look inflammatory and it’s easy to throw these patients on a steroid cream. But steroids make fungal infections worse, so if there’s any suspicion (based on scale or distribution), make sure. Or, if a patient comes back after being prescribed a steroid cream and it looks worse, consider an underlying fungal infection.
- Antibiotic: Impetigo, cellulitis, RMSF, secondary syphilis.
- Match the antibiotic to the most likely cause.
- For RMSF specifically, strongly consider starting doxycycline before lab confirmation if you truly suspect. Delayed treatment in the patients can be incredibly harmful.
- Supportive only: Viral exanthems.
- Most resolve within a week or two. For these, you just need to make sure you give the patient or parents clear follow up or return precautions.
Step 5: Know When to Follow Up and Refer
Patients should be re-evaluated (either with you or their PCP) after five to seven days of treatment. And refer to dermatology when:
- The diagnosis is genuinely unclear
- The rash is worsening despite appropriate treatment
- You’re concerned about an autoimmune or vasculitic process
- It’s chronic and not responding to standard care
Rash Morphology Breakdown
Here’s a closer look at each lesion type with common diagnoses and first-line treatment. This is also what the full Blox Rash Guide is built around, so if you want the visual version with clinical photos for each category, check out our free download.
Maculopapular Rashes

| Diagnosis | Key Features | Treatment |
| Viral exanthem | Pink/red rash with URI or GI symptoms, common in children, resolves in 1-2 weeks | Supportive |
| Drug eruption (morbilliform) | Symmetric pink rash 1-2 weeks after new medication | Stop medication, +/- steroids |
| Scarlet fever | Sandpaper-like rash, strawberry tongue, strep exposure | Penicillin or amoxicillin |
| Secondary syphilis | Symmetric rash including palms and soles, possible sexual exposure history | Penicillin G 2.4M units IM |
| Kawasaki disease | Fever more than 5 days, conjunctivitis, mucositis, extremity changes | Hospital for IVIG and aspirin |
| Roseola (HHV-6) | High fever resolves then rash appears on trunk spreading to limbs, common in children | Supportive |
Scaly Rashes

| Diagnosis | Key Features | Treatment |
| Tinea corporis | Annular lesion with central clearing and raised scaly border | Terbinafine 1% cream BID x 2 weeks |
| Tinea pedis | Scaling and fissuring between toes or moccasin distribution | Terbinafine 1% cream BID x 4 weeks |
| Tinea capitis | Scaly scalp patches, often with hair loss | PO terbinafine or griseofulvin x 6 weeks |
| Tinea versicolor | Hypo- or hyperpigmented fine scaling patches, especially on trunk | Ketoconazole 2% shampoo QD x 3 days |
| Eczema (atopic dermatitis) | Dry, itchy patches, often in flexural areas | Triamcinolone 0.1% cream BID |
| Psoriasis vulgaris | Well-demarcated silvery plaques, often on extensor surfaces | Clobetasol 0.05% BID + derm referral |
| Seborrheic dermatitis | Greasy scales on scalp, face, ears, chest | Topical ketoconazole |
| Pityriasis rosea | Herald patch then oval scaly lesions in “Christmas tree” pattern on trunk | Triamcinolone 0.1% cream BID |
| Secondary syphilis | Scaly reddish-brown lesions on palms, soles, and trunk | Penicillin G 2.4M units IM |
| Contact dermatitis | Scaly erythematous patches with known or suspected trigger | Clobetasol 0.05% BID, remove offending agent |
Vesicular/Blistering Rashes

| Diagnosis | Key Features | Treatment |
| Herpes zoster (shingles) | Painful grouped vesicles in a unilateral dermatomal distribution | Acyclovir or valacyclovir |
| Herpes simplex (HSV) | Painful grouped vesicles on erythematous base, perioral or genital | Acyclovir or valacyclovir |
| Bullous impetigo | Flaccid bullae, common in children, rupture easily | Cephalexin or dicloxacillin |
| Bullous pemphigoid | Large tense bullae +/- urticarial base, more common in elderly | Topical or PO steroids |
| Contact dermatitis (severe) | Itchy vesicles at site of irritant exposure, possibly linear | 4-week PO steroid taper |
| Stevens-Johnson Syndrome | Widespread mucocutaneous blistering, target lesions, often drug-induced | Hospitalization, supportive care |
| Dyshidrotic eczema | Small itchy vesicles on palms and soles, often chronic or recurrent | Clobetasol 0.05% BID x 2-4 weeks |
Pustular Rashes

| Diagnosis | Key Features | Treatment |
| Folliculitis | Small pustules surrounding hair follicles, tender or itchy | Topical mupirocin or clindamycin |
| Impetigo | Honey-colored crusts with underlying pustules, common in children | Mupirocin topically or PO cephalexin |
| Candidiasis | Bright red plaques with satellite pustules in moist or intertriginous areas | Topical clotrimazole or nystatin |
| Disseminated gonorrhea | Scattered pustules on extremities with fever and arthralgias | Ceftriaxone |
| Hidradenitis suppurativa | Painful nodules and pustules in axilla or groin, chronic and recurrent | Doxycycline 100mg QD, derm referral |
| Pustular psoriasis | Sterile pustules on erythematous base, may be widespread or localized to hands/feet | Consider hospitalization, urgent derm referral |
Petechial/Purpuric Rashes

This is the category that should get your attention, and you should have a low threshold for doing a deeper workup or faster referral on these patients.
| Diagnosis | Key Features | Treatment |
| Meningococcemia | Fever, toxic appearance, rapidly progressing purpura | Hospital, IV antibiotics |
| RMSF | Fever, petechial rash beginning on wrists/ankles spreading centrally, tick exposure | Doxycycline +/- hospital |
| Sepsis/DIC | Widespread purpura, ecchymosis, bleeding tendencies, systemically ill | Hospital, supportive care |
| HSP (IgA vasculitis) | Palpable purpura on lower extremities, abdominal pain, hematuria, often in children | Supportive +/- steroids |
| ITP | Petechiae and bruising, post-viral in children or chronic in adults, otherwise well | Supportive (mild), IVIG or steroids (severe) |
| Leukemia | Petechiae, pallor, fatigue, bone pain | CBC, urgent heme referral |
Targetoid Rashes
| Diagnosis | Key Features | Treatment |
| Erythema migrans (Lyme) | Expanding bull’s-eye lesion at tick bite site, 3-30 days after exposure | Doxycycline 100mg BID x 10 days |
| Erythema multiforme (minor) | Target lesions, often acral on hands and feet, no mucosal involvement | Topical steroids |
| Erythema multiforme (major)/SJS | Target lesions plus mucosal involvement, may follow infection or new medication | Hospitalization for severe cases |
| Toxic epidermal necrolysis (TEN) | Widespread skin detachment more than 30%, often medication-related | Hospitalization |
| Urticaria multiforme | Targetoid urticaria-like lesions in children, no mucosal involvement, triggered by viral illness or antibiotics | Antihistamine +/- steroids, stop offending agent |
Download the Full Guide
The tables above cover the major categories, but the full Blox Rash Guide goes deeper, with clinical photos for every morphology type, organized by location (trunk, extremities, intertriginous areas, hands and feet), and treatment mapped out for each diagnosis. It’s free and you can download it here.