
Between jammed fingers, falls, sports injuries, and work accidents, hand injuries are common in the outpatient setting. Many of them may look fairly minor at first, but there are a few important diagnoses that are easy to miss if you’re not mindful of them.
This post covers the hand injuries that show up regularly in outpatient practice that deserve a closer look.
If MSK injuries are something you’re still getting comfortable with, we’ll go much deeper into these kinds of cases inside our Blox Orthopedic Intensive. The first cohort starts April 7, 2026.
TL;DR
Purpose: Highlight several common hand injuries seen in outpatient settings that are easy to miss but important to recognize early.
Do this first: Start with the mechanism of injury and a focused hand exam. Many of the injuries that can lead to long-term issues are diagnosed clinically, even when imaging looks normal.
Red flags to look for:
- Inability to extend the DIP joint
- Inability to flex the DIP joint
- Small puncture wound over the MCP joint after a fight
- Thumb MCP instability
- Snuffbox tenderness after a fall
Initial checks
- Compare range of motion to the opposite hand
- Test individual tendon function (isolate the joint!!)
- Evaluate joint stability
- Assess neurovascular status
- Look for rotational deformity
First-line mindset: Not every significant injury looks dramatic. Some of the most important diagnoses present with minimal swelling, mild pain, or normal imaging.
Follow-up: If tendon injury, ligament injury, or occult fracture is suspected, immobilize appropriately and arrange follow-up evaluation with orthopedics.
Closed-Fist Injuries (“Fight Bite”)

Closed-fist injuries are one of the easiest hand injuries to underestimate.
A patient may present after punching something… or someone. Oftentimes they are vague about the details. The wound may be small and easy to miss, sometimes appearing as a small puncture over the MCP joint. Imaging is often normal, and the patient may say the pain is minimal.
The concern is that there may be a small puncture wound or break in the skin over a joint (particularly the MCP) that can introduce bacteria directly into the joint or extensor tendon sheath.
Human bites have a high infection risk, and even a small wound can lead to septic arthritis or tendon infection.
Key things to evaluate
- Location of the wound over the MCP joint
- Extensor tendon function
- Signs of joint involvement
- Mechanism of injury
Management considerations
- Antibiotics are usually indicated (Amox-Clav is a go-to)
- Careful wound evaluation is important
- Hand surgery consultation may be needed if joint penetration is suspected
The important takeaway is simple: if there’s any concern for an open wound over a joint, consider antibiotics and close follow-up with hand surgery or orthopedics. In areas with limited specialist availability, an in-office follow-up within 24–48 hours is warranted for a wound re-check.
Mallet Finger

Mallet finger is a very common sports injury and easy to miss if you don’t do a focused exam.
The classic mechanism is a ball striking the tip of the finger, often during basketball or football, causing forced flexion of the distal tip. The patient usually reports pain and swelling around the distal finger, and on exam they can’t actively extend the DIP joint.
This occurs because the extensor tendon insertion at the distal phalanx has been damaged. Sometimes there is a small avulsion fracture visible on X-ray, but the injury can also be purely tendinous.
Key exam finding: Inability to actively extend the DIP joint. The key point here is that you must isolate the joint in order to accurately check it.
Early diagnosis is important because treatment requires continuous DIP extension splinting. If the finger is allowed to remain flexed for an extended period, the deformity can become permanent.
Whenever you evaluate a distal finger injury, checking active DIP extension takes only a few seconds and can prevent a common missed diagnosis. Early orthopedic follow-up and patient education about staying in the splint is crucial.
Jersey Finger
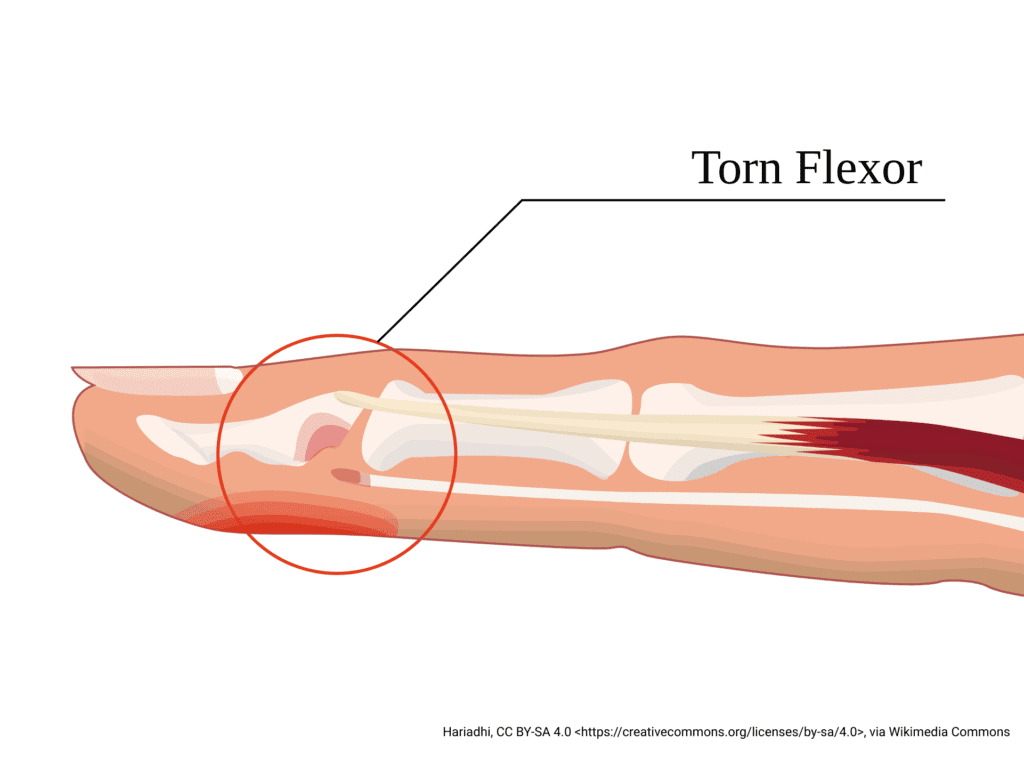
Jersey finger also often occurs during sports but is the opposite injury of mallet finger.
It happens when a finger is forcefully extended while the patient is trying to flex it. The classic example is grabbing another player’s jersey during a tackle.
Patients usually present with pain, swelling, and an inability to bend the tip of the finger.
This injury represents a rupture of the flexor digitorum profundus tendon.
Key exam finding: Inability to flex the DIP joint.
Unlike mallet finger, jersey finger almost always requires surgical repair. If the injury is missed, the tendon retracts and surgical repair becomes more difficult.
A simple exam maneuver helps identify this injury. Stabilize the middle phalanx and ask the patient to flex the tip of the finger. If they can’t, a flexor tendon injury should be suspected. Again, early orthopedic follow-up is key.
Thumb UCL Injury (Skier’s or Gamekeeper’s Thumb)
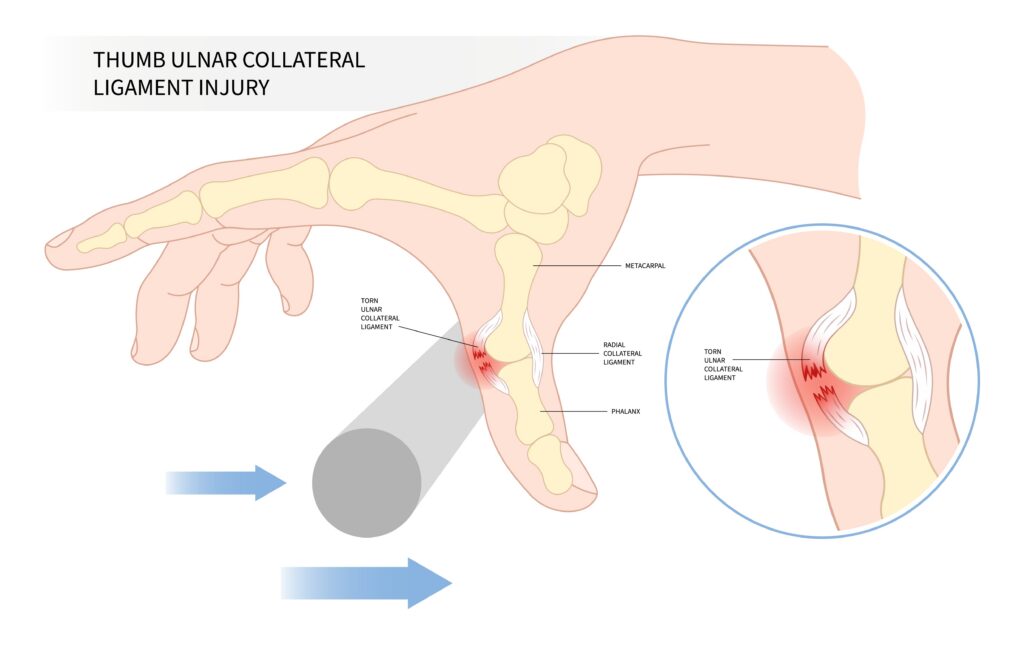
These injuries often appear minor but can significantly affect hand function.
The typical mechanism involves forced abduction of the thumb, often during a fall or sports injury.
Patients usually report pain and swelling around the MCP joint of the thumb. X-rays may show a small avulsion fracture, but imaging may also be normal.
The underlying issue is injury to the ulnar collateral ligament of the thumb MCP joint.
Key things to assess
- MCP joint stability (hold the metacarpal head in one hand and the proximal phalanx in the other)
- Test the unaffected side to compare stability
- Pain along the ulnar aspect of the thumb
- Mechanism of injury
If the ligament is completely torn, the thumb becomes unstable and grip strength can be significantly affected.
If you suspect this injury, the patient should be placed in a thumb spica splint and evaluated by hand surgery.
Scaphoid Fracture
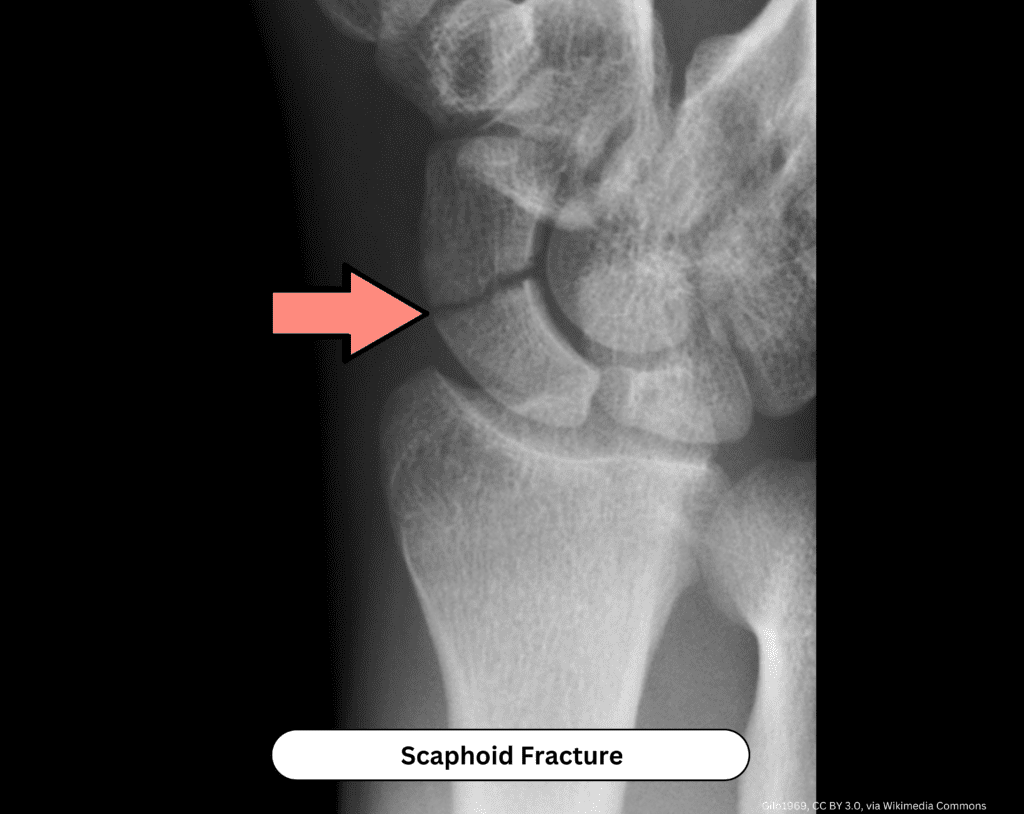
Scaphoid fractures are one of the most important wrist injuries to recognize early.
The typical mechanism is a fall on an outstretched hand (FOOSH). Patients usually present with wrist pain, with or without swelling, and initial X-rays may be normal.
The key exam finding is tenderness in the anatomic snuffbox.
Because of the scaphoid’s blood supply, missed fractures can lead to nonunion or avascular necrosis.
If clinical suspicion is high despite normal imaging, the safest approach is immobilization in a thumb spica splint with repeat or advanced imaging. The patient should follow up with orthopedics in 7–10 days.
Important point: When the mechanism and exam suggest a scaphoid injury, treat it as a fracture until proven otherwise.
Quick Reference: Hand Injuries Clinicians Can’t Miss
| Injury | Typical Mechanism | Key Exam Finding | Why It Matters |
| Fight Bite | Punch to mouth | MCP puncture wound | High infection risk, joint involvement |
| Mallet Finger | Ball strikes fingertip | Cannot extend DIP | Tendon injury requiring splinting |
| Jersey Finger | Forced extension while flexing | Cannot flex DIP | Flexor tendon rupture requiring surgery |
| Thumb UCL Injury | Forced thumb abduction | MCP instability | Loss of pinch strength |
| Scaphoid Fracture | Fall on outstretched hand | Snuffbox tenderness | Risk of nonunion, AVN, chronic pain |
Final Thoughts
Most hand injuries you see in clinic will be straightforward, but you need to be mindful of the ones that are easy to miss.
Taking a few extra moments to assess mechanism, tendon function, and joint stability can prevent many of the most common missed diagnoses. Always assess the unaffected side as well.
If MSK injuries are something you want to get better at managing, this is exactly the kind of material we spend time on inside our Blox Orthopedic Intensive.
We break down the exam findings, imaging, and decision making for the injuries you’ll see every week in clinic so you know what to look for and what to do next.
You can learn more and join the intensive here.