
Your first few sore throat patients as a new NP or PA can seem easy at first (especially if you get a positive rapid strep result before you even walk in the room). Then one of them has a muffled voice, neck pain, or trouble turning their head, and you realize not every sore throat is simple. Here’s what to watch for.
Fast Track Summary (TL;DR)
Purpose: Learn how to separate a basic sore throat from something that needs urgent attention.
Do this first: Use Centor criteria as a guide and always screen for red flags like trismus, drooling, neck stiffness, or respiratory distress.
Red flags:
- Muffled or “hot potato” voice
- Drooling or trouble swallowing
- Uvular deviation
- Neck swelling or limited motion
- Respiratory distress or stridor
Key takeaway: If your patient looks too sick for “just strep,” they probably are. Trust your gut and look closer.
A Reality Check: Patients Don’t Follow Textbooks
There’s a gap between what you learn in a textbook and how you actually approach patients once you’re out on your own.
Sore throats are one of the most common complaints you’ll see, but there’s huge overlap between viral, bacterial, and more serious causes. Subtle clues—like a voice change, posture, or how the patient swallows—can tell you more than the strep result alone.
Start Here: The Framework That Keeps You Grounded
Technically, you’re supposed to save strep testing for patients who meet Centor criteria. But in most clinics, your MA has already done a strep/flu/COVID swab before you even see the patient.
That’s fine and often helps speed up the visit, but your job is to look at the full picture, not just the test result.
If the rapid strep is positive and the symptoms and exam match, treat it. If it’s negative but your gut says otherwise, take another look and consider additional testing. This is where you start honing your clinical judgment.
✅ Sore Throat Quick Checklist
- Use Centor criteria as a guide, not a rule
- Expect rapid testing before you see the patient
- Always screen for red flags (voice change, drooling, trismus, stridor)
- If rapid strep is negative but suspicion is high, order a throat culture
- Consider mono, flu, COVID, or STI testing when the story doesn’t fit
- Reassess if symptoms don’t improve within 3–5 days
Breaking Down the Big Five
Here’s a quick reference for the most common sore throat causes you’ll see in urgent care and family practice:
| Condition | Key Clues | Management Focus |
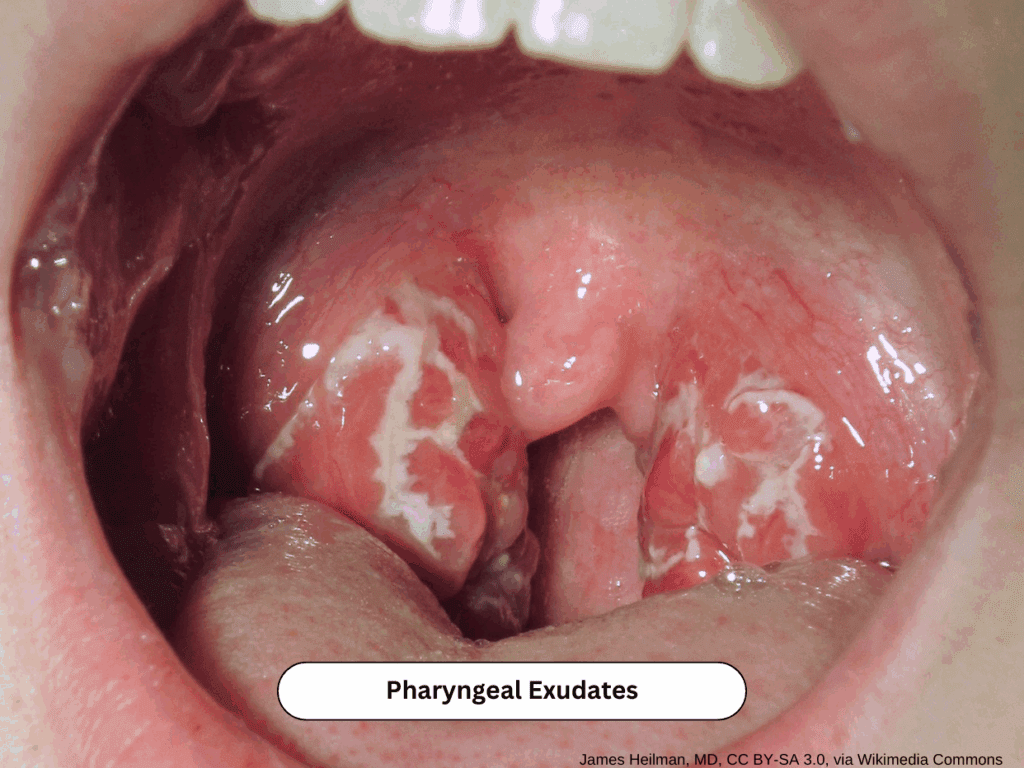
| Strep Pharyngitis | Sudden onset, fever, exudates, anterior cervical nodes | Rapid test or empiric antibiotics (Centor ≥3) |
| Viral Pharyngitis | Gradual onset, cough, congestion | Supportive care only |
| Mononucleosis | Fatigue, posterior nodes, amoxicillin rash with + Monospot | Avoid contact sports, no amoxicillin |
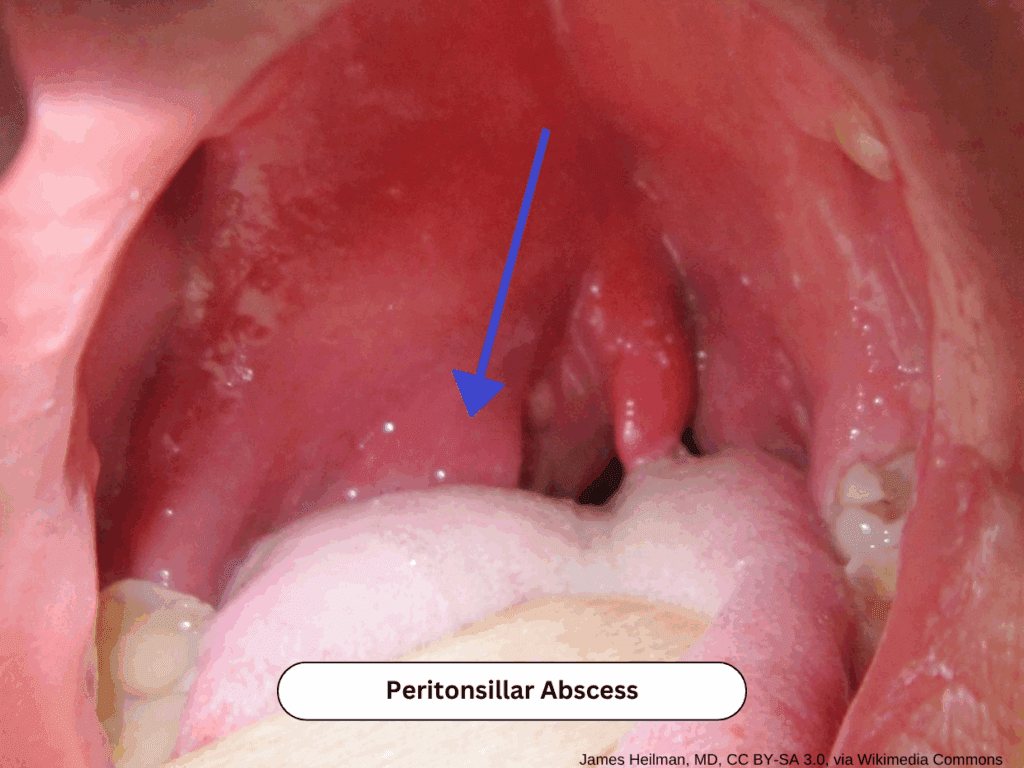
| Peritonsillar Abscess | Trismus, uvular deviation, muffled voice | ENT or ED for drainage and airway monitoring |
| Epiglottitis | Stridor, drooling, tripod position | Airway first, avoid throat exam, refer to ED |
Quick Pearls
- Rapid strep positive? Treat. Example: Penicillin 500 mg BID × 10 days (adults) or Amoxicillin 50 mg/kg (max 1000 mg) once daily × 10 days (kids).
- Rapid strep negative but high suspicion? Provide supportive care and send a throat culture. Consider additional testing if the patient is immunocompromised or just looks off.
- Symptoms not improving with antibiotics? Think about other causes like mono, gonorrhea, or peritonsillar abscess.
- Significant pain or swelling? A single dose of Dexamethasone 10 mg IM can help, but skip longer steroid courses.
The Red Flag Roundup
🚩 Immediate Concern:
- Drooling or muffled voice
- Stridor or respiratory distress
- Uvular deviation
- Neck stiffness or swelling
- Severe pain with minimal exam findings
The Bottom Line
Most sore throats are nothing to lose sleep over, but a few will surprise you. The more you see, the more you’ll learn to spot when something’s not right. Keep paying attention and trusting your gut, and you’ll catch the ones that matter.
And if you’re ever unsure what to do next, open Blox. The Pharyngitis topic walks you through testing, red flags, and treatment in seconds so you can stay confident and efficient.